Palmer Lucky is an evil fucking worm and dipshit beneficiary of government contracts. He’s the Oculus jackass with a shitty soul patch who runs a military defense company called Anduril. I could continue to talk about the general ways I dislike him on a personal level, but I’ll instead focus on a specific one: He shares many of my hobbies, including an enthusiasm for retro gaming and FPGA hardware. If you see the company ModRetro, know that’s his company. ModRetro recently released an FPGA-based machine in the shape of the N64 called the M64. You do not, under any circumstances, need to buy a war crime N64.
If I can be super petty for a second: the knob on that thing looks atrocious. You're mixing matte and glossy! Credit: ModRetro.
First let’s just talk about the practical: There’s no shortage of ways to play the N64. You can get original hardware and a CRT or an upscaler like the Retrotink, a piece of hardware that’s made by people who really care. You can also mod an HDMI port into an old N64 if you aren’t a coward. If you want something FPGA-based that plays cartridges, the Analogue 3D works. The Superstation One runs FPGA cores just fine. Or to hell with it, just get a MiSTer or even just download a god-fearing emulator. Nobody needs Palmer Luckey’s evil little device, particularly when the market has never been more saturated.
The Analogue 3D Works! Or get any number of MiSTer derivitives like the Superstation One! Or upscale your N64, or mod an HDMI port in there! There's so many ways to play the N64 these days. Credit: Wikipedia, Retrotink, MiSTer Addons, RetroRemake.co, Analogue,
This is not the first product ModRetro has put out. They also put an evil Game Boy out, and specifically put one out in “attack drone metal.” I hate these winking little shits. Not only are they using retro gaming to be fascists, they’re doing it in the corniest way humanly possible.
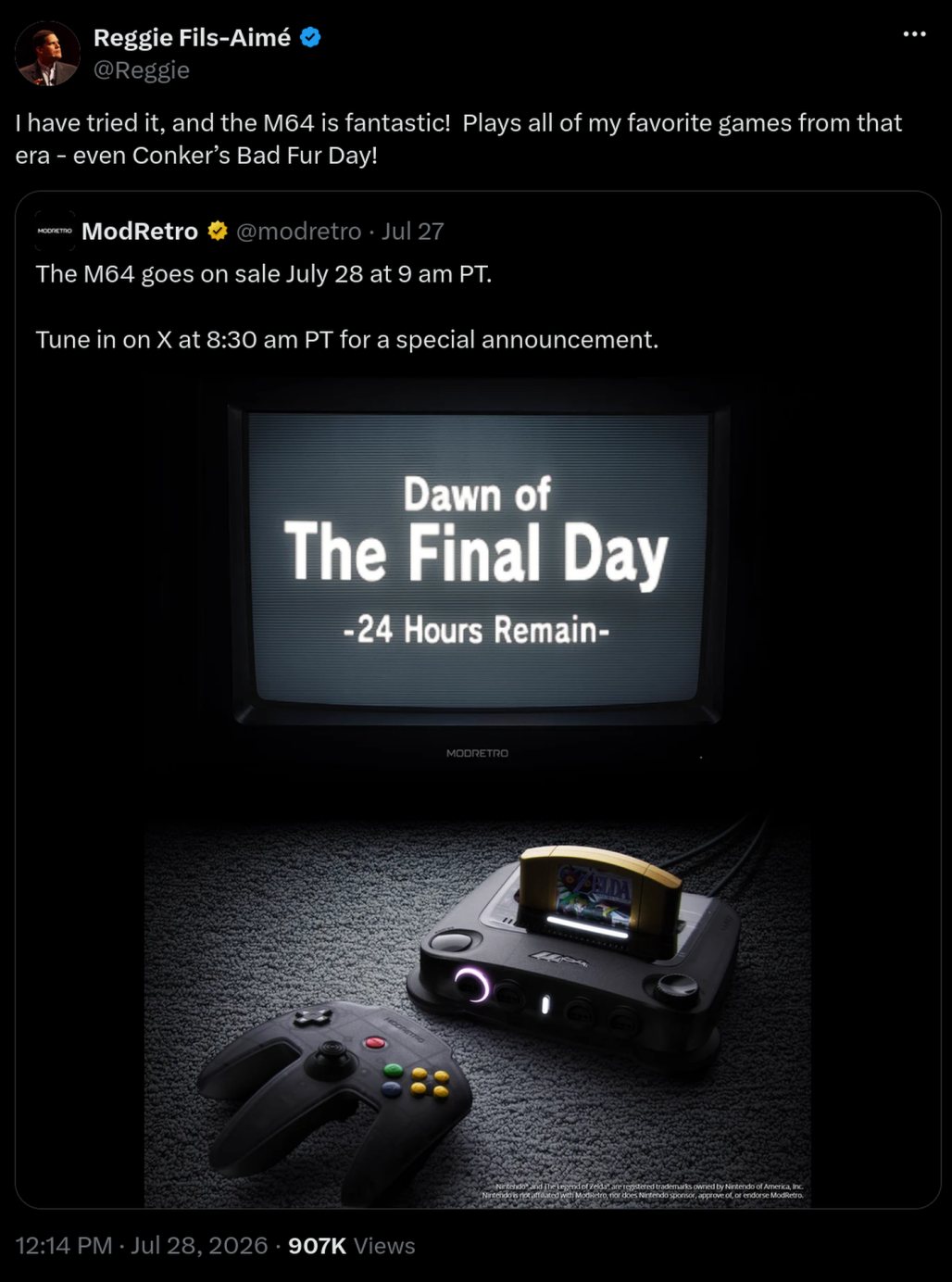
Former Nintendo of America President Reggie Fils-Aimé took to X, The Everything App twice in one day to signal boost that evil dipshit’s pet project. In the spirit of Hater Week, I’d like to officially state that Reggie can go fuck himself as well.
We cannot let these people feel comfortable in our hobby. Even if it’s just on a personal level, I’m sick of seeing them. The Video Game History Foundation’s Frank Cifaldi said it best last December: “I say this with zero irony: if you are even tangentially a part of a retro video game community, it is your civic duty to push back against this company and shun anyone who doesn't. This is fascism tapping gently at the door and as soon as you let it in, it's going to invite its friends.”
If we do not draw a line somewhere, they will continue to bring their hatred to us. There’s no better time than the present.
Palmer Lucky is an evil fucking worm and dipshit beneficiary of government contracts. He’s the Oculus jackass with a shitty soul patch who runs a military defense company called Anduril. I could continue to talk about the general ways I dislike him on a personal level, but I’ll instead focus on a specific one: He shares many of my hobbies, including an enthusiasm for retro gaming and FPGA hardware. If you see the company ModRetro, know that’s his company. ModRetro recently released an FPGA-based machine in the shape of the N64 called the M64. You do not, under any circumstances, need to buy a war crime N64.
“I was responsible for the dancing baby meme,” Rob Sheridan laughs over a video call. Now better known as an accomplished graphic designer and the former creative director of Nine Inch Nails, Sheridan’s list of accolades date back to 1997, when he created a website dedicated to the low-resolution animated GIF.
The first thing I notice when our interview begins is his t-shirt, which bears the ironic slogan “HOME TAPING IS KILLING MUSIC,” a phrase once printed on record sleeves in the UK during the ‘80s alongside a cassette tape resembling a skull and crossbones, later used in the logo of the infamous BitTorrent tracker The Pirate Bay. During his decades-long career in the music industry, Sheridan has stood out as one of the few outspoken advocates of media piracy.
“I was really early on the internet, making websites just as a hobby in high school to teach myself HTML,” he explains. “I remember the first time I was able to download the leak of a new song, Nine Inch Nails’ 1997 single ‘The Perfect Drug.’ It was played on a radio station and someone recorded it, and was able to upload it in this RealAudio format which compressed music in a way that made it manageable to download for the first time.”
While attending New York’s Pratt Institute the following year, Sheridan dove headfirst into the world of illegal file sharing. “Very much in the way that Napster originated, people had their own servers with files in public folders. You’d connect to the local network at your dorms and people had their mp3 collections on there. I ended up discovering a whole bunch of music that way. I downloaded a whole bunch of albums that I never had the opportunity to try because every album was an 18 dollar investment. That kind of radicalized me, and I became a fan of so much more music.”
While barely finished with his first year of art classes, a Nine Inch Nails fan site Sheridan had created caught the attention of the band, and in 1999 he was hired to design their official webpage.
“I ended up leaving school and moving down to New Orleans, living down at their studio and working there. One thing led to another and I became a creative partner, then art director, and doing more stuff,” he explains. “They'd all been kind of holed up in this studio for a couple years following up their huge album [The Downward Spiral], and it was all very secretive. I was the kid coming in with a bunch of energy and all this technological interest—like hey, check out this LimeWire thing. Everything we did with Nine Inch Nails was very confrontational with new technology.”
As an avid pirate suddenly finding himself in the midst of the music business, Sheridan saw the issue from a different angle than most of the suits he was surrounded by. “I got brought in and we were being flown to New York, the label was taking us out to these expensive dinners and paying for everything—top notch hotels, everyone had private cars and drivers. There was so much money going around, and it wasn't the artists who were rolling in cash. I remember one of my first comments to Trent [Reznor] was, ‘Now I see why CDs cost 18 dollars.’”
By the time Nine Inch Nails’ comeback album With Teeth hit stores in 2005, it had already been available to download on Oink for a number of weeks. Rather than joining the growing number of artists angry at their fans for not waiting to pay, Sheridan says they saw it as a failure on the side of the music industry. “We knew that the moment we sent it to the record label it was gonna leak. At the end of the day, Trent is a music fan too—if someone is like, ‘Hey, you can listen to the new album from your favorite band right now, or you can be good and wait three more weeks,’ of course you’re not going to wait. It's not really a moral question at that point. Instead of blaming them, we looked at the problem—which was the record label. That’s when we decided what we’re going to do is release the digital version first through our site, and then send it to the label. The CD can come out later.”
For the rollout of their next album, Sheridan and Reznor leaked singles via USB drives hidden inside the venues of their 2007 tour, kicking off a masterclass in viral marketing: an alternate reality game immersing fans in the dystopian future of Year Zero. Clues encoded in the mp3 files and tour merch directed participants to a string of websites and phone lines revealing further details of the album’s concept, music videos, cover art, and eventually the album in its entirety.
In October of 2007, Oink’s servers were raided by police and the website’s creator was arrested. The following day, Sheridan penned a eulogy for the website in a blog post titled The Death of Oink, the Birth of Dissent, and a Brief History of Record Industry Suicide, where he called the website “the most complete and most efficient music distribution model the world has ever known,” and added that he would gladly pay a large monthly fee for any legal music service of the same level.
The next year, Nine Inch Nails released their album The Slip for free via BitTorrent and direct download from their website, where Reznor wrote, “Thank you for your continued and loyal support over the years—this one's on me.” Though they weren’t the first major band to release an album for free during this era (Radiohead released In Rainbows via the pay-what-you-can model the previous year), this method marked the beginning of a change that would take the rest of the industry years to catch up to.
“It was us acknowledging how much of a download world it was, but it was also just continuing to experiment,” Sheridan says of the decision. “Part of that was acknowledging very early on that collecting your audience is very valuable. We got the email addresses of everyone that got it for free so that we could reach out to them about the tour that we were about to do, and sell tickets to that. Everyone was trying to figure out what their place was in terms of how to have an economy around music at that time. They had made music so expensive to access, while at the same time you've got Apple being like, ‘You can store a million songs in your pocket!’—okay well, I don't have a million dollars.”
Following Oink’s closure, record labels pressed on with business as usual, and a new private tracker called What.CD quickly sprung up to fill the void it left behind. In a short matter of time, the community would grow to match the vast library of its predecessor—a success which Sheridan sees as a product of the industry’s failure to adapt in an increasingly digital landscape. “I got on What.CD and kept rolling on there. It really was an answer to something that the music industry wasn't providing at the time. Now that’s kind of acknowledged by streaming music. It has a lot of major flaws, but kids today have no concept of how amazing it is. It should cost a lot more to be able to just flow through the entire history of music. You had to have been there in that private club to realize how special it is to have that access to music for everybody now.”
As exciting as this meticulously organized archive of free music was, I wouldn’t be able to invite my friends to let them join in right away. In order to acquire closely-guarded and highly sought-after invites, I would need to climb the rung of user classes to achieve the status of “Power User” by uploading a number of torrents myself. While at first it came off as unnecessarily elitist and gatekept in nature, the rules in place within the shadowy cabal of private trackers existed for a reason.
“If [trackers] are public and they're easy to get onto, that means they're also easy for law enforcement to get onto, so all they have to do is download the torrents and see who they're connecting to. Having a private site with some pretty hefty walls around it means that you are much more secure,” explains a former staff member and moderator of What.CD, who requested to go by the pseudonym ‘Brian’ during our interview.
“The other reason is that there’s no community on public sites,” he continues. “There are no accounts, there's no motivation really other than just your own goodwill, so it’s very common to download something and stop seeding it on your computer. Private trackers are built around having one account and one account only. They're built around tracking your ratio of upload to download. Those two things together provide a lot of incentive to continue seeding your content and making it available to other people. That’s what created the magic of private trackers being comprehensive and reliable.”
After passing the interview and becoming a member in 2010, Brian says his first impression of the website was something of awe. “Very quickly I understood what this site was—how much respect people had for it, and how much work it took to build and maintain. The community was very active on the forums and IRC,” he adds. “Still to this day, I've never seen such an actively maintained network of knowledge and output, it really sucked me in. Every band or album had a word cloud that showed connected artists, and I found a lot of music just by clicking around and optimistically downloading things. There were also the collages that people would make for their own personal taste, or by themes which ranged from, ‘Here are all the Pitchfork 10s,’ to, ‘Every album that has a train on the cover.’”
The following year, Brian became a staff member himself. “These places felt like some of the last survivors of the bulletin board style forums in a world that is now just Reddit and Instagram comments. There’s a real magic to that kind of communication. It was a lot of what I wanted in an internet community. I got involved on the interview team at the start. From there, they eventually asked if I wanted to handle more sensitive responsibilities and join the mod team.”
As a member of the mod team—the shadowy cabal within the shadowy cabal—Brian’s responsibilities mainly consisted of enforcing the rules surrounding user accounts, a task he says he handled when not occupied with high school homework assignments.
By this time, around 2011, What.CD had become the largest archive of music in human history. Taking the hard-earned lessons from their predecessor, the tracker had stayed under the radar of four-letter agencies. While operational security and potential legal action was always top of mind for staff, Brian says that during his tenure on the team, their largest perceived threat was a brief scare from the J.D. Salinger estate.
On What.CD, one of their most popular functions was the request system, a member-led bounty economy driven by the incentive of gaining valuable upload ratio. If a user wanted something that wasn’t already available on the website, they could create a “request” for it, offering a portion of their own upload credits to whoever was able to fulfill it. Typically, these requests could be filled by spending around $20 on Amazon or iTunes and uploading the files. For highly-sought after releases yet to hit shelves, other users chipped in on the bounty, creating a massive reward for whichever record store employee was willing to “borrow” a copy from the backroom before the release date, resulting in the website frequently becoming the originating source of album leaks online. The largest request on the website was for “The Ocean Full of Bowling Balls,” an unpublished short story by Salinger only known to exist in a locked room of the Princeton Library, where it was available by appointment to read under the strict supervision of staff.
“It was basically like a long running joke that it would never get filled,” Brian laughs. “And then somebody fucking did it.” In November of 2013, a What.CD user tracked down one of the 25 copies of the manuscript allegedly printed in 1999 in order to fill the request. The unexpected leak made headlines around the world, and the torrent file was quickly pulled. “It was known that the Salinger estate was very legally motivated, very litigious,” he says. “It would never be allowed to actually be on the website, so the hand was forced.”
While the unwanted attention raised alarms amongst staff, Brian says nothing came of it. “To the best of my knowledge, [action from law enforcement] never happened until the very end, and even that was pretty minor, but we were constantly paranoid about it. It was a huge thing on the back of our mind at all times.”
In November of 2016, users attempting to log into What.CD were shocked by a message displayed on the homepage, stating that, Due to some recent events, What.CD is shutting down. We are not likely to return any time soon in our current form. All site and user data has been destroyed. So long, and thanks for all the fish.
According to a French cybercrime website, authorities had seized a number of What.CD’s servers earlier that day. The sudden closure came as a surprise to their 165,000+ registered users, including staff like Brian. The site never returned, and no further details were ever made public to the mourning userbase. Even today, speaking about the loss of What.CD with an Anonymous stranger feels like recounting the death of a close friend.
“I feel like it’s probably okay to share the top level detail about this,” Brian says somberly. “What.CD’s security was very strong. It was run by very smart people who knew their stuff about being systems operators. Ultimately, some servers in the network were taken down by a French enforcement arm. They were just reverse proxies, which didn’t store anything actually sensitive, except maybe a connection that led to the real servers. That was the first and only time—that I'm aware of—that any kind of enforcement had been launched against the site. Even though nothing happened, even though there is a world where we could have just replaced the server and switched all the hosting in that country to something else and continued onward, the admins made the very reasonable decision to say, We are now in a different sector of risk, we’ve gone from zero actions taken to one action taken, we’re abandoning ship—and started deleting everything. There was no way of knowing whether they would follow the trail to the next server. It was obviously a very difficult decision and the admin I talked to after was really upset about it, but I'm sure many people agree it was also the sensible choice to make.”
Coinciding with the shutdown, streaming services had begun to reach the masses. As CD sales continued to plummet, labels moved away from physical releases, and major leaks became increasingly infrequent. Suddenly, anyone with a $10 monthly subscription had access to the entire world of music without even having to download it to their hard drive. In the wake of What.CD’s closure, I begrudgingly became a paying Spotify user. The record labels had finally won the war against music piracy.
Looking at the state of things now, much of what Sheridan predicted in his 2007 blog post has come true. Music has more or less become free, and we finally can pay a nominal fee for a service once offered only by illegal websites like Oink. Reflecting on his thoughts from nearly two decades ago, Sheridan isn’t so certain that we’ve arrived in a promised land.
“The idea at the time that music will eventually be free was more of a statement of where this is heading. Streaming is not economically sustainable for artists. The solution to all of this should have also been something that renegotiated how artists are paid for music. Instead, you've got artists who can’t even afford their bills even though they’re getting millions of streams a month, and you have Spotify paying Joe Rogan 100 million dollars. Artists are the ones being mistreated, while the middlemen are making a ton of money. There’s this whole world where people exist just to show up in the middle and take a big chunk of the money from something they had no part in creating. The Spotify model is like saying your favorite restaurant should just be giving you free food until you decide to buy a t-shirt. If artists weren’t also being screwed on the touring side, then you could think of streaming as marketing, but there’s too many examples being dangled in front of our face of how much money is being funneled away to billionaires and corporations, and artists always come last. That’s my frustration with where we’ve ended.”
One thing I realize now being an old Gen X'er is that even when you spent a lifetime trying to build the world that you wished for, reality has a way of making it suck as bad as when you started.
"“The idea at the time that music will eventually be free was more of a statement of where this is heading. Streaming is not economically sustainable for artists. The solution to all of this should have also been something that renegotiated how artists are paid for music. Instead, you've got artists who can’t even afford their bills even though they’re getting millions of streams a month, and you have Spotify paying Joe Rogan 100 million dollars. Artists are the ones being mistreated, while the middlemen are making a ton of money."
The Presidential 1776 Award competition was set up by the Trump administration to honor the U.S.’s 250th birthday with a civics contest for high school students.
But the family of Aangad Singh, 15, believes he may have been kept out of the competition’s final because of his Sikh background and visible turban, NOTUS reports.
Singh, a rising high school junior who lives in Connecticut, entered the competition in February just like other high school students around the country. He scored well enough to reach the finals in Washington, D.C., at the end of June and make the final eight. But his elimination after that left his family—and many of his competitors—puzzled.
The Singh family didn’t think Aangad had done poorly, but there wasn’t a live scoreboard. Other contestants told them after the competition that they were sure Aangad had won and were shocked that he wasn’t in the top three. When Aangad’s mother, Ramandeep, asked an official with the Department of Education, which helped run the contest, for the final scores, the official told her that was proprietary information.
So, the Singh family waited until the competition was televised on CBS three weeks later, and Aangad was shocked to learn some of his correct answers were labeled wrong.
In one instance, Aangad was asked to give four examples where federal courts have jurisdiction as outlined in Article 3 of the Constitution.
Two of his answers—“Parties of state and citizens of another state,” and “Case with state and foreign nation”—were marked wrong. He showed his father a copy of the Constitution showing that his answers were right.
In another instance, during a lightning round, Aangad was asked “Which amendment ended slavery?” and his answer was marked wrong. Initially, he thought his pronunciation of “Thirteenth” was bad and that his th- sounded like an f. But he was reassured when the TV subtitles proved that he said the correct answer.
After the round ended, each contestant was interviewed by host Mario Lopez before he announced the three finalists, and Aangad gave an answer about being proud to share his knowledge about the country’s founding principles. Then, he watched white contestants from Michigan, Washington, and Wyoming be announced as the winners.
Singh’s family thought that he was robbed, and weighed taking action. To his mother and uncle, it seemed like Aangad was being kept out of the spotlight—and a visit to the Oval Office to meet President Trump—because he was a brown kid with a turban. They didn’t care as much about getting a share of the $250,000 in scholarship money as much as Aangad being recognized for his hard work.
The Wyoming winner was a homeschooled girl who would later be touted by the Department of Education for culture war propaganda, and the Washington state winner told Trump at the White House she wanted to attend Hillsdale College, a politically conservative school, to which Trump said he could give a recommendation.
Aangad’s father, Bhalindar, reached out to the Department of Education twice by email, but has yet to get a response. The Education Department told NOTUS that the questions in the competition were “developed, judged, and scored independently by the James Madison Memorial Fellowship Foundation.” NOTUS sent the foundation a detailed list of questions, but also hasn’t heard back.
Minutes before NOTUS’s deadline, the Department of Education responded, saying that the competition’s rules stated that judges would “exercise independent good faith judgement” in selecting finalists and winners, and that, by participating, contestants “agree that the decision of the judges is final and binding.”
For those old enough to remember, Michael and Robby Meeropol will always be the Rosenberg boys.
I never knew them as such, but it’s not hard to imagine what they were like, in part because there are so many pictures. In one, from June 1953, they are sitting outside the White House in shirts and ties, wool coats, and Brooklyn Dodgers caps. Six-year-old Robby holds his grandmother’s hand; to his right stands a rabbi.
The boys look uncomfortable, and solemn. Their parents, Ethel and Julius, have been convicted of spying for the Soviet Union and sentenced to death. Robby and Michael are there to ask President Dwight Eisenhower to spare their lives. Michael, who is 10, has written a letter that he will hand to a White House guard: “Please let my mommy and daddy go and not let anything happen to them. If they come home Robby and I will be very happy we will thank you very much.”
Out of the frame, but documented in other photos from that day, are the placards that protesters carried invoking Robby and Michael, the helpless boys made symbols of what many believed was a grave injustice about to be perpetrated against their parents. (Counterprotesters, carrying signs saying FRY ’EM and HANG ’EM, disagreed.) Similar scenes played out around the world. After Pope Pius XII called for clemency, the Vatican’s newspaper cited the “two little innocents on whose soul and destiny the death of their parents would forever leave sinister scars.”
I learned the broad outlines of the events that followed—the electric chair, and the orphans it left behind—half a century later, on a weekend visit to the home of my parents’ friends Robby and Elli in western Massachusetts. I was 8. I don’t recall how the subject came up or exactly what I was told, but I remember trying to picture the electrocution, and that I couldn’t sleep that night. I knew Robby mostly as the kind of adult who enjoys making bad puns and funny faces for kids’ amusement. The notion that, as a kid himself, he had been orphaned by the United States government didn’t seem to match his playful persona. I wondered, but didn’t quite know how to ask, how anyone could go on living after something like that had happened. And how could he possibly seem so normal?
I later learned more: that Robby and Michael had been adopted after the executions, taken a new last name, and all but disappeared from the public eye. They went to college and graduate school, got married, had children of their own—only to reemerge as public figures in the 1970s, vowing to clear their parents’ names. From then on, they’d never really stopped talking about Ethel and Julius, or pressing the government for answers about its evidence and motivations for seeking their death. By the time I was old enough to observe their advocacy firsthand—at a public event commemorating the executions’ 50th anniversary, and later in a presentation Robby gave at my high school—I understood their basic posture to be one of resolute protest. Ethel and Julius, they maintained, had not been atomic spies. They had been scapegoated for their political allegiances, framed by prosecutors, and wrongfully killed.
This was not, I came to understand, an uncontroversial position. One year, my family’s Yom Kippur break-fast meal was very nearly derailed when my dad got into an argument with one of our guests about the Rosenbergs. Julius and Ethel, this guest insisted, were both guilty as charged, and to pretend otherwise was a pinko fantasy. The incident left me with yet more questions about my parents’ friend and the complicated historical legacy he’d inherited.
I’ve lately been able to ask Robby and Michael many of these questions directly—and to go beyond the abbreviated, textbook version of their family’s story, deep into the countless primary and secondary sources that, for nearly 75 years, have helped shape an ever-evolving debate about what, in this case, constitutes truth, and what justice really means. The facts are messier and more resistant to facile conclusions than either side of the argument might care to acknowledge. Even now, new ones continue to emerge.
Christopher Churchill for The Atlantic; Julius and Ethel Rosenberg collection at the Howard Gotlieb Archival Research Center, Boston University Libraries
Michael ( left ) and Robby with items from the Rosenberg papers at Boston University, more than 70 years after the executions
Since the fall of the Soviet Union 35 years ago, government files have been declassified and grand-jury testimonies unsealed; key players have made dramatic confessions. Robby and Michael, the old men who were once such young boys, have had to make their own sense of these revelations. Not all of them have been easy to accept.
In April of last year, I spent a day with the brothers in Cold Spring, New York, where Michael and his late wife, Ann, moved in 2009. The town sits on a hill overlooking the Hudson River, and I got off the train from New York City that morning with hikers who fanned out to the nearby trails.
Robby was waiting to pick me up at the station in his red Toyota; he’d arrived early, as he is apt to do. On the short drive to Michael’s condo, we made easy small talk. I’d made clear that the article I was writing would be solely mine to shape, and they’d agreed that I could ask them anything. But I knew that once I turned my recorder on, I’d need to ask questions that might put me in league, in their minds, with the legions of other journalists they believed had fixated on the wrong angles, or missed the point of the Rosenberg case entirely.
Before I started reporting this story, I’d met Michael only in passing. We’d now talked on the phone a few times, and my main takeaway was that his being a retired economics professor made a lot of sense. His tendency was to carefully (and loquaciously) argue a point, and he had limitless enthusiasm for wading into the minutiae of legal details and chronology. Robby, by his own admission, preferred to focus on more general themes. As the three of us sat talking in Michael’s living room, Robby pointed out that his brother, being four years older, had spent far more time with their father than he had. Robby seemed to think of Julius more as a historical figure he happened to be related to, while Michael, on some level, still mourned the father he’d lost as a 10-year-old.
Julius was a co-owner of a struggling machine shop on the Lower East Side. On weekends, he would take Michael to ride the New York City subways and elevated trains for hours on end; they would stand at the very front, where they could look out at the switching tracks. Ethel stayed home with Robby. She worked hard at being a good mother—she sang to her boys, read Parents’ magazine, took a class in child psychology. In their small apartment near the Manhattan Bridge, the kids shared the lone bedroom while their parents slept in the living room.
Listening to Michael’s descriptions, you could almost forget that his early years were different from those of other postwar American kids: “I’d have a wooden baseball bat and a Spalding ball or a tennis ball. He”—Julius—“would pitch it to me, and I would hit it.” Michael was listening to The Lone Ranger on the radio when, one July night in 1950, FBI agents came to the door to arrest his father.
In his letters from jail and later prison, Julius tried to reassure his sons. “Don’t you worry,” he wrote; “we’ll be playing games again as soon as I can straighten out this trouble I’m in.” But on August 11, after Ethel appeared before the grand jury that had indicted Julius and refused to answer any questions, she, too, was arrested. Neither of them ever came home again.
After his mother’s arrest, Michael told an aunt that he wanted to run into the street and get killed by a car. He stopped eating. He drew endless railroad tracks, switching and merging and looping but going nowhere. When he complained to his grandmother Tessie Greenglass, with whom he and Robby were staying, she told him to send Ethel a telegram. But he didn’t want to upset his mother, so he said that he was “having a nice time. I miss you very much. Love, your son, Michael.”
The boys were eventually sent to the Hebrew Children’s Home in the Bronx, where attendants beat and ridiculed children. To Robby, it felt as if he and Michael were imprisoned, just like Ethel and Julius. He didn’t understand what his parents had been accused of doing. Instead, he harbored an anxious sense that some menacing force had broken up his family—and stood ready to do more damage if given an opening. He would try to avoid attracting attention, lest “they” take notice and wreak more havoc. He also developed a coping mechanism that I sensed had become a lifelong habit: “Whenever something was really bad,” he told me, “I always figured out some way to say, Oh, it’s no big deal. It’s not happening. It’s a form of denial, I guess.”
As I watched the brothers that day in Cold Spring, they struck me as, above all, brothers—by turns affectionate and peeved with one another, as likely to use a childhood nickname as to sigh in exasperation. They are fluent in the vigorous conversational cadence of older Jewish men raised in mid-century New York. “Verbal combat,” Robby later said, was a favored family pastime. But neither of them seemed eager to undergo much emotional probing.
At one point that afternoon, Michael spent a few minutes recounting the songs his parents had played for them as kids, enjoying himself as he quoted what Julius had called “nonsense” lyrics from “Oh! Susanna” and other “camp songs.” If not quite fully transported back in time, he appeared willing, at least, to try going there.
Without meaning to, I broke the spell. As Michael began to reflect on his relationship with Ethel, and his sense that he’d been a “bad boy,” frequently misbehaving, I tried to prompt Robby to add his own recollections from that pre-arrest period. “I don’t know,” Robby said, and paused. Maybe it was too much to expect a 3-year-old to have formed clear memories. In any case, he quickly changed the subject back to their decades of advocacy work.
Before I boarded my return train to New York City, Michael reminded me to look out the window on my left. A few stops away, in Ossining, the barbed-wire fences and high turrets of Sing Sing towered over the tracks. In opting to spend his retirement near his grandkids, Michael had ended up living half an hour from the site of his parents’ deaths.
Robby and Michael visited their parents in prison for the first time in the summer of 1951, after more than a year apart. By then, the boys had gotten used to the Hebrew Children’s Home, and then they had gotten picked up from it. Now they were staying with their “Bubbie,” Sophie Rosenberg, who played with them and cooked foods they liked. Still, they were eager to see their parents again.
Julius and Ethel were separated in prison, allowed to see each other only once a week or so. Mostly, they communicated through letters. Anxious to put the boys at ease, Julius wrote to Ethel that he planned to draw them pictures of trains, boats, and buses. “Hah! You can’t make me jealous with your boats and trains,” she replied. “I have an envelope full of rare specimens collected with painstaking care by that intrepid hunter of wild insects, namely, your wife!” She worried that Robby in particular “may be a little shy and strange with us.”
In another letter to Julius, Ethel imagined how they might explain their situation to the boys. “Of course, we feel badly that we are separated from you but we also know that we are not guilty and that an injustice has been done to us by people who solved their own problems by lying about us,” she wrote. “It’s all right to feel any way you like about them, so long as your feelings don’t give you pain and make you unhappy.”
At Sing Sing, the boys saw Ethel first, then Julius. Determined to prove his fearlessness, Michael asked to see the electric chair for himself. Ethel had suggested that Julius describe its effect as “painless electrocution,” similar to “a highly magnified electric shock that anybody might sustain.”
“The fact is both children are disturbed,” Julius wrote after the visit.
Bettmann / Getty
Robby and Michael visited their parents in prison for the last time on June 16, 1953.
Bettmann / Getty
Ethel and Julius Rosenberg in a police van after their conviction
The executions had been set for May 1951, but the date kept getting pushed back as appeals made their way through the legal system. On subsequent visits, all four Rosenbergs were allowed to be together, and the mood of their reunions became lighter. As a family, they laughed and sang songs; sometimes, they played hangman. When Michael asked his parents if they were truly innocent, they assured him that they were.
“You boys are our greatest pleasure and joy in life and we love you more than anything else in the world,” Julius wrote in one letter. And indeed, it’s hard to read the letters, and the various accounts of these visits, and come to any conclusion other than that Ethel and Julius loved their sons. They agonized over the details of the boys’ care and cursed the government for separating them.
But it’s also hard not to question why they didn’t do more to prevent their sons from being orphaned—why they chose not to take advantage of the numerous opportunities they were given to cooperate with the authorities, and to live.
Ethel’s younger brother David Greenglass made a different choice. When Klaus Fuchs was arrested by the British in early 1950 for passing atomic plans to the Soviets, his testimony led American authorities to Harry Gold, a chemist. Gold in turn led them to David, who had been a machinist at Los Alamos during World War II, and his wife, Ruth.
The Greenglasses quickly confessed that they had been part of a spy ring led by Julius Rosenberg, through whom they said they had shared sketches of the atomic bomb’s design with the Soviets in 1945. Ruth said that Julius had told her to recruit David, and that Ethel was there and had been encouraging.
The FBI was certain that Julius had more valuable information, and hoped that he would confess and name names, just as his brother- and sister-in-law had. But Julius denied everything, and refused to point a finger at anyone else. So J. Edgar Hoover decided to adopt a recommendation from a subordinate, who wrote that agents should “consider every possible means” to make Julius talk—including bringing charges against Ethel. Hoover wrote to the attorney general: “Proceeding against his wife might serve as a lever.”
The Greenglasses’ testimony gave the government enough evidence for an arrest warrant. But like Julius, Ethel told the authorities nothing—nor did her arrest have the intended effect on her husband. The trial, though, brought out new testimony from the Greenglasses, who said that Ethel hadn’t just been a supportive bystander, but had typed up David’s hard-to-read notes on classified atomic science. Now the death penalty seemed like a real possibility for both Rosenbergs.
At the sentencing, Judge Irving R. Kaufman said that he considered the couple’s actions “worse than murder”—a crime with untold numbers of past and future victims. Russian access to the atomic bomb, Kaufman said, had “already caused, in my opinion, the Communist aggression in Korea, with the resultant casualties exceeding 50,000 and who knows but that millions more of innocent people may pay the price of your treason.” Kaufman made clear that both husband and wife were to blame. “Julius Rosenberg was the prime mover in this conspiracy,” he said, but Ethel was a “full-fledged partner.” Both therefore deserved to die.
Subsequent revelations from multiple prosecutors in the case have shown that the judge didn’t come to this conclusion entirely on his own. Roy Cohn, who was an assistant U.S. attorney on the case, later said that prosecutors had had clandestine phone conversations with Kaufman, “especially about whether Ethel should be sentenced to death.”
The Rosenbergs’ co-defendant, Morton Sobell, a former classmate of Julius’s at City College, also claimed total innocence. Sobell was convicted of conspiracy to commit espionage and sentenced to 30 years in prison (he was spared the death penalty because no evidence tied him to sharing atomic secrets). David was sentenced to 15 years in prison and served less than 10. Ruth, who was never charged, stayed with their two young children.
A few weeks before their deaths, the Rosenbergs were visited at Sing Sing by James V. Bennett, the director of the Bureau of Prisons. Bennett said he’d been sent by the attorney general with an offer: If they were ready to talk, officials would recommend clemency.
Ethel was outraged. “I made it short and sweet,” she wrote to her lawyer. “I was innocent, my husband was innocent, and neither of us knew anything about espionage.” What right did the government have “to try to forcibly wring from us a false confession, by dangling our lives before us like bait before hapless fish! Pay the price we demand, or forfeit your lives, is that the idea?” Bennett pleaded with her to change her mind.
The deputy attorney general later said of Ethel, “She called our bluff.”
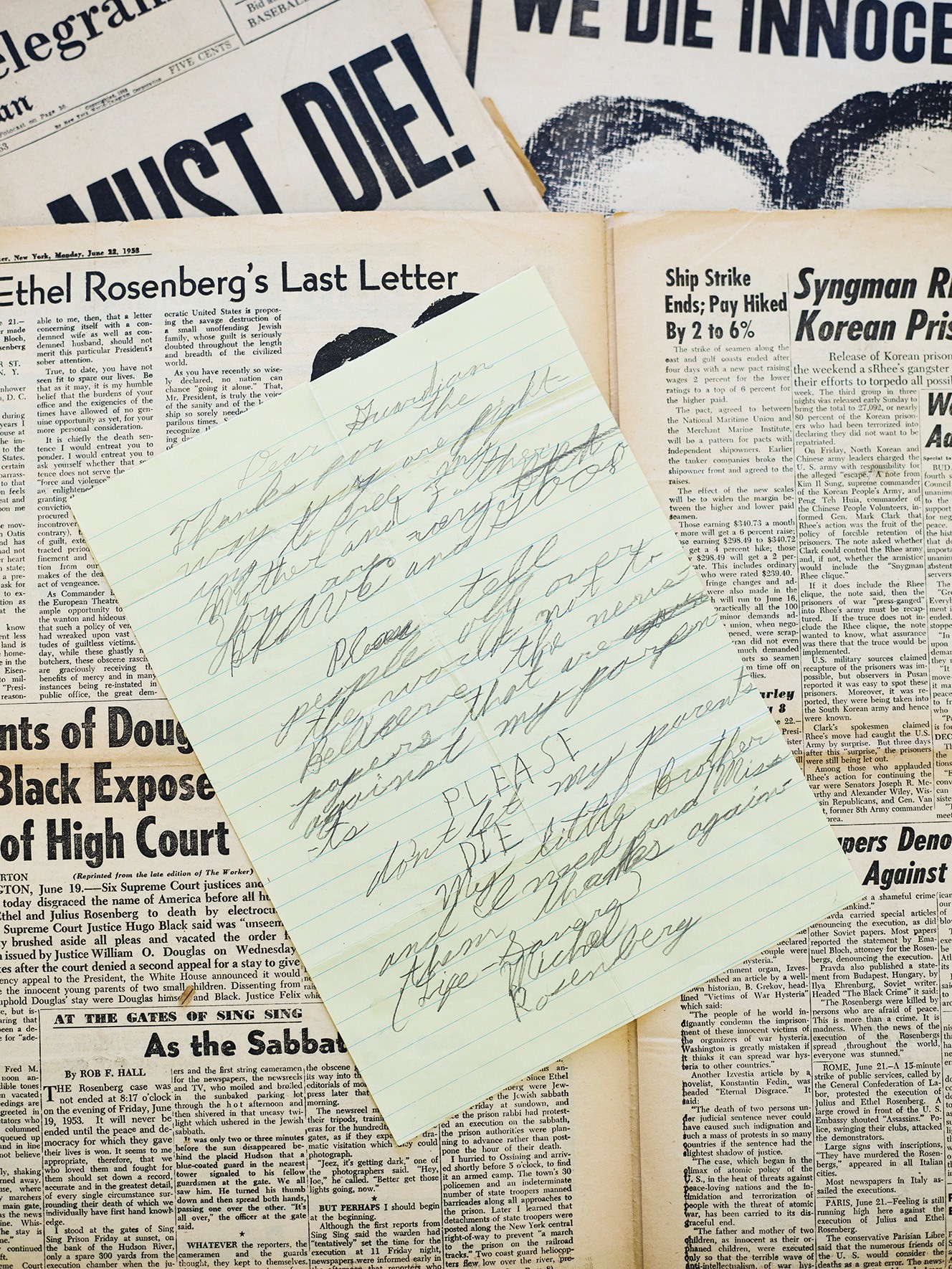
In June 1953, the day after their 14th wedding anniversary, after several last-minute appeals—including to the U.S. Supreme Court—had failed, Julius and Ethel Rosenberg, ages 35 and 37, had one final afternoon together, separated by wire mesh. Ethel wrote a letter to their sons that they would both sign: “We wish we might have had the tremendous joy and gratification of living our lives out with you,” it said. “Always remember that we were innocent and could not wrong our conscience. We press you close and kiss you with all our strength.”
The letter would have a much wider audience than just Robby and Michael, who were by then living with family friends in New Jersey. The uncertain fate of the Rosenbergs had become global news, and the couple’s letters were being distributed in dozens of countries via pamphlets and newspapers. From December 1952 to June 1953, 80 rallies in support of the Rosenbergs were held in Paris alone. One French diplomat told Secretary of State John Foster Dulles that the case was “the most troublesome issue affecting relations between the United States and Europe.”
Christopher Churchill for The Atlantic
“PLEASE don’t let my parents DIE. My little Brother and I need and miss them,” Michael wrote in a letter to a left-wing weekly.
Last summer, Robby, Michael, and I visited the archives at Boston University’s library, where many of their parents’ prison letters are housed. As we looked through the collection, Michael said that, when it comes to his mother’s letters, he considers only two or three “really real”—that is, not written for public consumption. He has returned to one of these often.
Two days before the scheduled executions, Robby and Michael visited their parents for the last time. Michael left crying and screaming: “One more day to live, one more day to live!” But Ethel didn’t cry. Later, she tried to explain her behavior in a note she sent her sons via her lawyer. To show emotion “would have been so easy, far too easy on myself,” she told them. “I took the hard way instead of the easy, because I love you more than myself and because I knew you needed that love far more than I needed the relief of crying.” She continued:
I know, sweethearts, an explanation of this kind cannot ever substitute for what we have been missing and for what we hope to be able to return to, nor do I intend it as any such thing. Only, as I say, we need to try to remain calm and free from panic so that we can do all we can to help one another to see this thing through!
Just after 8 p.m. on June 19, Julius followed Sing Sing’s Jewish chaplain to the electric chair. As the rabbi prayed, the executioner secured the five leather straps. Before he delivered the fatal shocks, he put a leather face mask on Julius meant to prevent his eyes from popping out of his head. Julius was pronounced dead after he received three charges of electricity.
The rabbi then gave Ethel a final chance to live. Did she have any names to share? She said she did not: “I’m innocent; I’m prepared to die.” She was strapped in and masked. The executioner delivered three shocks. But doctors found that the three charges had not been sufficient; Ethel’s heart was still beating. It took two more jolts, and four and a half minutes total, to kill her.
Michael and Robby were watching a baseball game on TV when a news flash came on the screen announcing that their parents were about to be executed. The adults sent the boys out to play ball with friends. By the time they came back in, they were orphans.
I first read Robby’s memoir, An Execution in the Family, soon after it was published, in 2004. I was 11 then, and gripped by the kid’s-eye perspective of the early chapters. I retained two distinct mental images from the book. One was of the Hebrew Children’s Home. The other was of a train set, which served as a partial answer to the question of how the boys could have turned out as well-adjusted as they had; there was, strange as it sounds, a happy part of this story.
On Christmas Eve 1953, the boys went to a party at the home of W. E. B. Du Bois, who had advocated for clemency for Ethel and Julius. Inside the largest house the boys had ever been in was an enormous Christmas tree with a pile of presents underneath it, all for them. This was where Michael and Robby first met Anne and Abel Meeropol, who asked them that night if they wanted to move in with them. Their own two sons had been stillborn, and Anne and Abel, now in their 40s, wanted badly to be parents.
By the start of 1954, Robby and Michael were living with the Meeropols in Manhattan; the couple were fun and loving, and the boys quickly began calling them Mommy and Daddy. But one night in mid-February, after Robby had gone to sleep, New York City police officers knocked on the door of the couple’s apartment to demand that he and Michael be turned over immediately.
Ethel and Julius’s lawyer had died of a heart attack before he could legally transfer guardianship to the Meeropols. Now two child-welfare groups had obtained a court order to remove Michael and Robby from the Meeropols’ home, on the grounds that living with former Communist Party members was not in the boys’ best interest. Abel refused to open the door and, in Michael’s telling, informed the officers that, if they wanted to take Robby and Michael, they’d have to kill him first. Somehow, he and Anne were able to arrange with lawyers to keep the boys overnight.
The next day, a judge ruled that Robby and Michael should be considered wards of the state and sent them to an orphanage. But the day after that, the Meeropols and Sophie Rosenberg, the boys’ grandmother, appealed to the New York Supreme Court, which gave Sophie temporary custody. For the next several months, Robby lived in fear of being sent back to the orphanage. Eventually, in September 1954, he and Michael were allowed to return to the Meeropols’. Recounting this turning point as we pored over the archives at Boston University, Michael began to cry. Anne later told him, he said, that she and Abel had plans to flee to the Soviet Union with the boys if they were not granted custody.
Michael and Robby started using the Meeropol name almost immediately, allowing them at last to slip back into private life, and they were formally adopted in 1957. The family’s Washington Heights apartment was, as Michael and Robby remember it, always full of laughter, music, and funny voices; it had room for all of their toys, including a Lionel electric train set. The boys kept huge tanks of fish and had a cat named Fuzzy Shnooky Romeo. When Robby went away to camp, Abel drew him cartoon postcards with silly, smiling animals. “Daddy got us worms!” the fish exclaim in one. “Yum! Yum! Hooray!” Abel signed the postcards “Pop.” Robby still has them.
Christopher Churchill for The Atlantic; courtesy of the Meeropol family
In 1954, Robby and Michael went to live in Manhattan with Anne and Abel Meeropol, who later became their adoptive parents.
Both Abel and Anne had been public-school teachers; Abel had taught James Baldwin high-school English. Abel was also a songwriter—in the 1930s, he’d written the music and lyrics to “Strange Fruit,” a song about lynching made popular by Billie Holiday—and had been successful enough that the couple could now live primarily off his royalties, in effect serving as full-time parents.
Anne and Abel rarely brought up the past with Michael and Robby, but when Ethel and Julius did come up, the Meeropols reinforced their sons’ impression of them as brave, principled people who had been wrongly executed. As they grew into adulthood, Michael and Robby came to treat that final letter from June 1953 as gospel: Always remember that we were innocent and could not wrong our conscience.
In the years immediately following his parents’ executions, Michael said, he didn’t cry at all. But when he was 16, a work of fiction—a 1947 novel by Willard Motley—finally cracked the defensive shell he’d developed. In his journal, he wrote:
I read the end of Knock on Any Door which describes a man’s feelings as he goes to his death in the chair. It shook me, and it broke me. I realized that the two dearest people in the world to me had gone through that agony and more. They probably worried about their “babies” and what would happen to them. My God was it awful. I cried and cried and cried so much. I feel terrible.
Oh to be half as courageous as those two wonderful people—Ethel and Julius Rosenberg. MY GOD
Abel saw him crying, and saw what he’d been reading, and gave him a long hug.
More than their childhood, Robby and Michael wanted to talk with me about the chapter of their lives that began in the 1970s, when they chose to “come out” as Rosenbergs after years of keeping quiet about who they were.
One night in early 1973, Michael heard that a trial lawyer named Louis Nizer, who had not been involved in the Rosenberg case, was reading out loud from his parents’ prison letters on TV. Nizer had just published a popular book about the case, The Implosion Conspiracy, which concluded that the Rosenbergs were guilty as charged. Michael called Robby, upset. The brothers believed that they held the copyright to their parents’ letters, which they saw as their sole inheritance. Why should Nizer be allowed to use them for his own biased ends?
On June 19, 1973, the 20th anniversary of their parents’ deaths, they filed a lawsuit. “We are strongly reaffirming our identification with and respect for our murdered parents and what they did for us both in their role as citizens as well as in their relationship with us as parents,” they wrote. It wasn’t long before the press showed up. “All of a sudden we were public,” Robby recalled. “And the sky didn’t fall.” In some ways, it was liberating to no longer be keeping such a big secret.
The legal bills were expensive, and they began traveling around the country to raise money, giving speeches under the auspices of a new National Committee to Reopen the Rosenberg Case. They planned to use the Freedom of Information Act to obtain the government’s evidence, or lack thereof, about their parents. In 1974, Robby stood onstage at Carnegie Hall and declared, “In the next year we are going to blow the lid on this case.”
Touring the country, they met well-wishers who were emotional about seeing “the boys” as grown men, people who cried and hugged them and hung around a little too long. Robby and Michael found this draining. Their preferred approach relied more on logic than emotion. They vowed to follow the facts. They would become experts; they would make an unimpeachable case. They wouldn’t get carried away by anger or grief.
Still, revisiting the letters and reading the trial transcripts for the first time forced Michael to relive the pain of his parents’ deaths, he told me. Publicly, he remained composed, but in private, for a year or so, he “cried, cursed, raged,” struck anew by the pathos of his parents’ correspondence and the could-have-beens of their complex appeals process. By the late 1970s, the brothers were exhausted by the work of being professional Rosenbergs, and starting to worry that the effort was futile. Their FOIA lawsuit had yielded hundreds of thousands of documents, but there was no smoking gun—maybe there never would be.
Sometimes, Robby and Michael told me, they wondered if there might be more to their parents’ story than what was in their letters. They never questioned that Ethel and Julius had been framed as atomic spies, but could they have committed some lesser offense that had made them government targets? Yet whenever the brothers asked Morton Sobell, their parents’ co-defendant, to tell them the truth, all they got was the same one-line answer: They were innocent.
With the collapse of the Soviet Union, rumors started trickling out of Russia: According to erstwhile KGB agents now speaking openly for the first time, Julius Rosenberg had in fact been a spy, and a valuable one. But Soviet intelligence operatives aren’t anyone’s idea of reliable sources, and it was easy for Robby and Michael to brush their claims aside.
In July 1995, the U.S. government released a series of previously classified documents known as the Venona files. These decrypted Soviet communications from the 1940s told a similar story to that of the former KGB agents: Julius, along with Ruth and David Greenglass, had spied for the Soviet Union. The headlines crowed with the certainty of a fresh verdict: “NEW EVIDENCE PROVES COUPLE WERE SPIES, OFFICIALS SAY.”
To Robby and Michael, suddenly seeing their parents in the news again as spies was painful. The whole thing felt like a disaster—“like a ton of bricks,” as Robby put it to me. In a joint statement, they suggested that the NSA and the CIA had “cooked” the evidence to frame their parents. Venona, they insisted, changed none of their conclusions. One official release was not going to be enough to undo years of deep suspicion of the government.
Still, Robby and Michael parsed the new evidence carefully. The files, they noticed, contained only one mention of Ethel: She was politically aligned with her husband and aware of his activities, the decrypted text said, but “in view of delicate health does not work.” This seemed like an important clue. If you interpreted “work” to mean “spy,” as Robby and Michael did, that would suggest the damning typing story was pure invention on the Greenglasses’ part.
Ruth Morgan / New York Daily News Archive / Getty
Ethel’s brother David Greenglass told authorities that he had been part of a spy ring led by Julius Rosenberg.
Slowly, more clues emerged. In 1999, a former KGB agent published a book revealing findings from Soviet archives that had briefly been opened a few years earlier. This, too, implicated Julius as a spy. Then, in a 2001 TV interview, David Greenglass (who had been living under an assumed name since he got out of prison and appeared on the program in disguise) admitted that he’d lied on the stand when he said that Ethel had typed his notes. “I don’t know who typed it, frankly,” he said. “To this day, I can’t even remember that the typing took place.”
Greenglass did not express remorse for having sent his sister to her death, citing her “stupidity” for not cooperating with authorities. He said his conscience was clean. When the interviewer asked him what he would say to Robby and Michael, whom he had not seen since they were children, he replied, “I’m sorry that your parents are dead.”
Morton Sobell was the one person who could definitively answer Robby and Michael’s questions about their parents. He had been Julius’s friend since they’d met as engineering students at City College. He had stood trial with both Rosenbergs and, after getting out of prison in 1969, stayed in touch with Robby and Michael.
For nearly six decades, Sobell maintained his innocence. But in 2008, at the age of 91, he told a reporter that, yes, he and Julius had turned over military secrets to the Soviet Union during World War II. If you wanted to call that spying, then sure, they’d been spies. Ethel, he said, had known what Julius was doing. “But what was she guilty of? Of being Julius’s wife.” Robby and Michael felt as though, for the first time, a trusted source had stated it plainly: Julius was a spy, and Ethel was not.
The brothers were shocked by Sobell’s sudden admission. They had asked him again and again to tell them the truth about their parents, even if only in private. Why had he lied? Michael still thinks about this, he said: “What if Morty had been honest with us?” He could have spared them so many years of uncertainty.
Even so, the brothers told me that finally learning the truth was a relief. They were in their 60s by then—both grandfathers—and had had more than a decade to consider the information in Venona. They now understood that their parents’ prosecution hadn’t been a senseless witch hunt, as they’d once believed. Ethel and Julius hadn’t been targeted randomly, or simply for having been Jewish Communists during the McCarthy era. And because Sobell himself had been the one to say it publicly, Robby and Michael wouldn’t have to do the uncomfortable job of breaking the news to the remaining Rosenberg true believers, who still thought that any talk of spying was a government hoax.
I was taken aback by their matter-of-factness. Was that really it? Could their ultimate reaction to learning that Julius had spied for the Soviet Union have been gratitude that they didn’t have to be the messengers? I wanted to know how they felt about the actual spying—about the fact that their father had shared highly classified information in order to aid another, later hostile, country’s militarization, destroying their family in the process.
When I pressed them on this, Michael and Robby conceded that perhaps Julius had been, as Robby put it, “kind of a cowboy,” prone to taking big risks without much concern for the effect they might have. Maybe, Michael suggested, a more responsible choice for a spy would have been to not have children at all. Nonetheless, they both remain sympathetic toward their father, and continue to argue that he was unfairly prosecuted. Even if Julius was a spy, they maintain, he was not an atomic spy, and as such was not guilty of the charges for which he was executed.
Julius seems to have approached his spying with a sprightly, if naive, enthusiasm. He was 24 and working as a junior engineer for the Army Signal Corps in New York when he was recruited by Russian agents in 1942, drawn to the promise of helping defeat Hitler and the notion, however fanciful, that the Soviet Union represented a solution to America’s social ills. He went on to provide thousands of documents containing valuable military-industrial information, and became an active recruiter. His Soviet handler Alexander Feklisov recalled in his memoir that Julius could sometimes “be as carefree as a teenager,” such as when he greeted the Russian during an early street-corner meeting with a hearty “Hello comrade!” On another occasion, Feklisov wrote, Julius told him that, although he loved his wife and son (this was before Robby was born), his meetings with Feklisov were “among the happiest moments of my life.”
Unlike Julius, Ethel was never given a code name in Venona, which Michael and Robby took to mean that she was not a spy. Why, then, should she have sacrificed herself, leaving her sons behind, particularly after Julius was executed and she was given one last chance to cooperate? Why did she choose death?
The question nagged at me for months; no single explanation—psychological, political, or otherwise—felt completely satisfying. Part of me wanted to see Ethel as a victim, caught between her husband’s recklessness, the vindictiveness of powerful men who didn’t care whether she lived or died, and the fear that she was already too far down a path of deception to allow the world, let alone her sons, to learn the messy truth. I thought about the toll that years of what was essentially solitary confinement, as the only woman on death row, would take on anyone; it seemed likely that she was not, by the end, thinking rationally. But that way of looking at it denied Ethel agency. It was possible, of course, that she’d made the choice to die of her own free will—as a martyr for the Communist cause, to make the United States look bad, out of loyalty to Julius.
When I raised the subject with Robby and Michael, they readily agreed that Ethel could have saved herself, had she wanted to. “She did have names,” Robby said. “In fact, if she’d given the names of Sarant and Barr”—Alfred Sarant and Joel Barr, members of the spy ring who had already defected to the Soviet Union—“nothing would have happened.”
“So should she have?” I asked.
Both brothers replied immediately and emphatically. “Oh no,” Michael said. “I don’t see why,” Robby added. Making any choice other than the one she ultimately made, they argued, would have left Ethel with a permanent sense of guilt over turning on her husband and reversing her steadfast commitment to “see this thing through”—the battle she’d been waging, and the story of innocence she’d been telling her sons and the world for three years.
“Mom could’ve said, I knew Julius was a spy; I helped him a little bit. I knew the names of two of the people he worked with. That’s all I know; take it or leave it,” Michael said. “They would’ve taken it.”
“Who knows,” Robby muttered, but Michael’s counterfactual scenario seemed plausible enough to me, and I let him keep talking as he imagined what might have happened next.
“She would have served some time in prison, and repudiated her marriage, and repudiated all the people who had supported them, and pulled the rug out from under Rob and me when they said that ‘we were innocent.’ And then shown up in our lives.”
I knew he was trying to explain why this never would have worked. But even if their mother reappearing in their lives at a later date might have proved complicated, it was hard for me to believe that it would truly have been worse than not having her in their lives at all. “We might have grown up to hate her,” Michael continued. He wasn’t sure he could have forgiven her for turning on his father—or for exposing the reality, while she was still alive, that both parents had lied to their sons. “The thought of her living that life was so horrible that I think it was easier to just follow him into the grave.”
Michael seemed to be saying that by admitting her dishonesty, Ethel would have ruined their childhood and poisoned any prospect of a future relationship with her. But wouldn’t some people see the fact that she’d died for a story she knew was false—something the brothers were acknowledging—as a greater betrayal? Michael and Robby didn’t seem willing to think about it that way. In their telling, Ethel had died, at least in part, to protect them.
Hulton Archive / Getty
Ethel at her arraignment in August 1950
For the brothers to wish for any other outcome would be for them to wish for an entirely different life than the one they’ve had and, against all odds, mostly enjoyed. It would be to wish that they’d had a childhood with no Meeropols, and an adulthood with more secrecy, less purpose. Faced with something—someone—so ultimately unknowable, perhaps the best that anyone can do is decide on their own version of the truth and stick to it.
I am not, I realize, the first to raise these contradictions. The ghost of Ethel Rosenberg has haunted American life for decades, by turns exasperating and enthralling those—psychiatrists, playwrights, novelists, scholars, journalists, relatives—who have tried to wrap their arms around the meaning of her life and death.
Few today would dispute that the government’s case against Ethel was less than airtight. In 2015, after David Greenglass died, his 1950 grand-jury testimony was unsealed. “I said before, and say it again, honestly, this is a fact: I never spoke to my sister about this at all,” Greenglass had said. If that was true, then he had likely perjured himself when later, at trial, he gave the evidence that led to Ethel’s conviction and sentencing. To some, Ethel’s alleged encouragement of David’s recruitment is evidence enough of her active role in the conspiracy to commit espionage of which she was found guilty. But Robby and Michael argue that knowledge of a conspiracy is not the same as participation in it—and that the prosecution failed to produce any proof she did participate, beyond what came directly from the Greenglasses’ unreliable accounts.
Whether or not you believe that the Rosenbergs deserved to die, there’s no denying that the punishment they received was unusually severe. Harry Gold was convicted of conspiracy to commit espionage and got out of prison in time to work as a clinical chemist in a Philadelphia pathology lab before he died at 60. Ruth Greenglass confessed to being a courier at Los Alamos and never spent a single night in jail. And, indeed, the case against Ethel was especially thin.
All of this ought, I think, to count for something in any honest assessment of the legal and ethical validity of the Rosenberg verdict. But I wasn’t sure that the injustice of the whole affair was enough to explain, logically or morally, the clarion confidence of Ethel’s claim that “I was innocent, my husband was innocent, and neither of us knew anything about espionage.” That was a lie.
Last summer, I visited Robby in western Massachusetts, where we sat in his sunny home office as his elderly gray cat threatened to knock over our water glasses. On the wall next to Robby’s desk, I noticed a calendar from the Union of Concerned Scientists. The cartoon for that month showed a uniformed military official lounging coquettishly on a bed, phone in hand. The caption read: “No, you dismantle your nuclear arsenal first.”
Other walls displayed framed mementos from the Rosenberg Fund for Children, the nonprofit Robby started in 1990 that supports the children of progressive activists who have lost their livelihood, been discriminated against, faced prison time, or died as a result of their activism (my parents have been longtime supporters of the RFC). Pointing to the images in his office, Robby told me that the organization has allowed him to connect with hundreds of kids and teenagers who can relate to what he experienced. They have sometimes asked why he’s not angrier. His response has always been that he considers his work to be a form of “constructive revenge.”
“My taste in vengeance is more intellectual than physical,” Michael wrote in the ’80s. Talking with him in the 2020s, I could see what he meant. Rather than cause for frustration, it seemed to be almost a source of comfort that there will always be another thread in the Rosenberg case to pull—more documents to uncover, more verbal combat to undertake.
Over the past decade, Robby and Michael have made a concerted push for Ethel’s exoneration. In December 2016, the brothers again stood outside the White House, this time to deliver a petition asking President Obama to exonerate their mother in light of the newly released grand-jury testimony. They held a photograph of themselves there as boys, delivering the plea to Eisenhower that went unanswered. This one did, too.
But a newly declassified document released toward the end of Joe Biden’s presidency once again gave them hope. In September 2024, the brothers received a copy, via their lawyer, of a handwritten 1950 memo by Meredith Gardner, the chief Venona code breaker. If the Venona files represented Gardner’s translated decryptions of the original Russian messages, this document, they believed, showed his own takeaways from those decryptions, and were thus a better reflection of the U.S. government’s top-level findings. Gardner wrote, for example, that Ruth Greenglass was known “to have been a Soviet agent.” Just below that are his notes on Ethel:
MRS. JULIUS ROSENBERG—A message of 27 November 1944 stated that Mrs. Rosenberg was a party member, a devoted wife, and that she knew about her husbands work, but that due to ill health she did not engage in the work herself.
Unlike the earlier releases, which stated only that Ethel did not work, this one specified that she did not engage in the work—the spying.
To Michael and Robby, this was the smoking gun that they had spent 50 years hoping to find. The first time they read the memo, they told me, they high-fived; Michael cried. They called on the Biden administration to exonerate their mother. Again, they were disappointed.
One virtue of Julius and Ethel having been dead for nearly three-quarters of a century is that their sons will never have to confront them about what they now know; one difficulty is that they will never get to. This impossibility seems to act as a kind of buffer. They can shake their heads at their father’s actions and tell themselves that their mother did the only thing she could, while reserving their deepest outrage for the one actor they still have the power to wrangle with: the United States government.
On several occasions over the course of my reporting, Michael brought up the petition that he and Robby had tried to deliver to Obama in 2016. Still eager for a reply, Michael sent a letter to the Obama Foundation in Chicago in the spring of 2025, and then another—by certified mail—to the foundation’s office in Washington, D.C. He never heard back.
Recently, Michael told me that he had given up on trying to elicit a response from the former president. “I thought it was a bigger deal than other people did,” he admitted. Robby, for his part, told me he preferred to look forward, not back. He is 79 now; his brother is 83.
But Robby didn’t mean that he was ready to stop thinking about his parents’ deaths or fighting for his mother’s exoneration—only that he didn’t want to waste any more time on old strategies that hadn’t panned out. The brothers are working with Representative Jim McGovern, Robby’s congressman, who last year made a floor speech in the House about Ethel and has advocated for her exoneration. They’d love to see a major Hollywood movie about their mother, they said, to reignite public interest in the case.
Listening to them, I thought about the train tracks Michael had drawn as a kid, endlessly looping back on themselves. Where, if anywhere, might these latest efforts lead? In some ways, the brothers have gotten much further in their quest than they ever anticipated they would; their deep satisfaction at the 2024 release of the Gardner memo came not just from its contents, but also from the somewhat improbable fact that they lived to see it, after 50 years of requests and lawsuits and petitions. It had given them a sense of forward motion, and a measure of vindication late in their lives. They knew far more than they once had. How could they stop now?
This article appears in the August 2026 print edition with the headline “The Rosenberg Boys.”
Back in February, Trump FCC Boss Brendan Carr launched a fake “investigation” of ABC because the network’s comedians and daytime talk show hosts hadn’t adequately kissed Republican ass.
“Since then, the ABC talk show hasn’t featured a single political candidate running in a competitive midterm race, according to a Semafor analysis.”
Earlier in the year, Republicans were upset that The View hosted Texas Democratic hopeful James Talarico. That triggered an entire fake “investigation” and a threatened revocation of ABC’s broadcast licenses by Carr, who falsely claimed that the daytime talk show had violated the FCC’s dated and irrelevant “equal time” rule requiring that TV stations give equal time to political candidates from both parties.
The threat of annoying costly legal headaches were still apparently enough to scare ABC (and likely other outlets) away from hosting politicians who would be critical of Trump.
It’s a shame that ABC, which had previously started to show some a signs of life in its battle with the thin-skinned U.S. president, suddenly doesn’t really want to talk about why The View rejected requests to host NYC Mayor Zohran Mamdani, or the democratic socialist candidates he supported for Congress, Darializa Avila Chevalier and Claire Valdez:
“A spokesperson declined to provide Semafor with a comment about how the show was reacting to the inquiry but has previously said the show is a “bona fide news program” and therefore isn’t subject to the equal time rule.”
Carr, you’ll recall, also threatened San Francisco area AM radio station KCBSlate last year simply for reporting on local ICE activity, resulting in the station demoting one anchor and softening its political coverage overall. Carr also tried (and failed) to censor and fire comedian Jimmy Kimmel after the late night host made a joke about deceased right wing propagandist and racist Charlie Kirk.
That said, avoiding politics entirely for fear of losing money is fairly common across corporate media (including outlets like Semafor), resulting in no shortage of pseudo-journalism that pulls its punches, particularly when it comes to being honest about the continued Republican descent into bigotry and fascism.
President Trump and Congress are neither investing in long-term solutions nor offering short-term relief. If they paid attention to different indicators of Americans’ financial health, beyond top-line growth and other traditional measures of economic success, they might feel more urgency.
So we developed one: a model budget for a family of two parents and two children under 8. We set their annual income at $130,000 — well above the roughly $83,500 national median for all U.S. households, and right in the middle of the income distribution for a family of four.
According to our calculations, the math has stopped adding up for this family over the past 18 months. They had a small cushion in 2024. Now they are in the red after covering just the basics, such as housing, an Affordable Care Act marketplace health care plan and day care. The family has over $1,000 less than it did a year and a half ago. Rising costs have more than wiped out any gains from higher wages and recent tax cuts.
This family would have trouble paying for anything beyond the basics — say, a car breaking down or a kid breaking an arm. It could not budget for any of the things that a typical family might hope for: buying a new car, taking a summer vacation or welcoming a third child.
To mount an effective response, it helps to know what stresses Americans feel most sharply and what action they expect from their elected officials. So we asked people.
By almost four to one, Americans told us that rising prices, rather than paychecks that haven’t kept up, are driving a cost-of-living squeeze. Two-thirds say they are struggling today and need relief they can feel right away. And the most cited concern is grocery costs. Some 35 percent of Americans in our survey, which we conducted last month, identified food as the single biggest source of financial pressure — approximately 15 percentage points higher than the share who named housing, the second-most-chosen option.
Several things are going on here:
First, kids, and in particular small children, are incredibly expensive in this country, because the Bible says that it’s wrong to take money from the rich to help pay the child care costs of ordinary people.
Only slightly less facetiously, I read a piece somewhere recently in which a partner at a big law firm told a woman associate that he considered choosing to have a child like choosing to go on a round the world sailing trip, that is, an act of extraordinarily extravagant consumption. It’s a real mystery why birth rates are now well below replacement level in any country where women have any economic and social freedom.
Second, it’s really hard psychologically to adjust for inflation, especially for older people as I know from experience. $130,000 per year sounds like a really big income to me because 30 years ago it WAS a really big income (equivalent to $282,000 today). But now it’s only the median income for families of four. We’ve discussed the psychology of inflation quite a bit at LGM, and it’s a difficult political issue for all sorts of reasons.
Third, a bunch of expenses that are very heavily subsidized or socialized altogether in the developed world — child care especially, but also health care and higher education — aren’t in the US, because of the Bible and Confederate Jesus and Elon Musk.
Fourth, and related, even people with moderate to quite high incomes in the US are laboring under the constant and growing pressures of economic precarity, because of the Bible etc.
Fifth, housing costs vary wildly across the country, so $130K per year for a family with two young kids might be plenty of money in Ashtabula, but barely middle class in Pasadena (of course you’re living in Pasadena rather than Ashtabula but this is in many cases not really anything like an actual choice given where the jobs that pay that kind of money are).
Sixth, the Bible.
There’s also some interesting discussion in the piece about how the price of meat in particular is a huge burden for many people, which is a problem that has at least a superficially obvious solution, but I’m pretty sure the right to bear cheeseburgers is somewhere in the Constitution so maybe not.